
Hepatic Epithelioid Hemangioendothelioma Treated With Irreversible Electroporation and Antibiotics:a case report
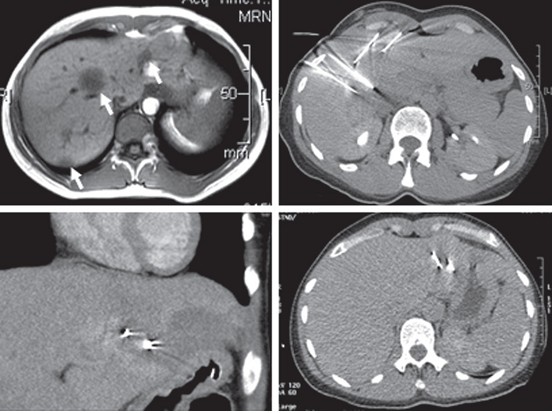
A 36-year-oldwomanpresented with transient right upper quadrant pain. Hepatic lesions were noted using ultrasound followed by computed tomography (CT), magnetic resonance(MR)imaging, and positron emission tomography (PET) scans; dual-echoMRexamination of the patient’s abdomen revealed multiple hypointense lesions (Fig 1A, arrows) and multiple subcentimeter nodular lesions in both lungs.Aseries of biopsies revealed a proliferation of cords and nests of vessels that were immunoreactive with CD31 and CD34. The lining endothelial cells were epithelioid in appearance and contained single to multiple vacuoles. Nuclei were irregular and showed some hyperchromasia, with few mitoses observed. There was an adjacent sclerosing tissue reaction. The histologic features were those of HEHE. Polymerase chain reaction analysis of the biopsies and blood samples revealed Bartonella genus bacterial DNA,9 as well as the reciprocal t(1;3)(p36;q25) translocation. The patient elected serial CT monitoring, during which tumor progression was noted. Following this, treatment of the tumor nodules was performed with IRE, and the Bartonella infection was treated using antibiotic therapy.
For the infection, the patient underwent a 12-month regimen of both rifampicin 600 mg and azithromycin 500 mg per day. This was followed by 4 months of rifampicin 450mg per day and doxycycline 100mg twice per day for an additional 3 months the following year.
A series of IRE procedures was performed
with institutional ethics approval and informed consent from the patient. The
first procedure was designed to ensure the safety of the system, and was therefore
only targeted to treat the largest lesion, in liver segment 4, as visible in
Figure 1A (middle arrow). Treatment was performed under general anesthesia. The
electrodes were placed through a series of transintercostal insertions (Fig 1B) under
CT and ultrasound guidance. Aneuromuscular blockade was perfused to attenuate
electrically induced muscular contraction, and electric pulses were delivered
using the NanoKnife electric pulse generator system (AngioDynamics,
Table 1.IRE Procedure Pulse Parameters
|
Procedure |
Date |
Lesion |
Segment |
Dimensions (cm) |
Electrodes (No.) |
Total Sets (No.) |
Average Separation (cm) |
Average Voltage-to-Distance Ratio (V/cm) |
Exposure Length (cm) |
Average Current (A) |
|
1 |
May 6, 2009 |
1 |
4 |
8.0 × 5.2 × 5.2 |
5 |
10 |
2 |
1,330 |
2 |
45 |
|
2 |
June 2, 2009 |
2 |
8 |
4.9 × 5.2 × 6.5 |
3 |
8 |
1.6 |
1,350 |
2 |
47 |
|
3 |
July 21, 2009 |
3 |
2/3 |
3.7 × 2.8 × 2.3 |
2 |
7 |
1.3 |
1,690 |
2.3 |
25 |
|
4* |
Aug 12, 2009 |
4 |
6 |
2.0 × 1.9 × 1.9 |
2 |
2 |
1.2 |
1,780 |
2 |
25 |
|
|
|
5 |
5 |
3.0 × 3.0 × 3.0 |
2 |
3 |
1.2 |
1,670 |
2 |
31 |
|
5 |
Dec 20, 2011 |
6 |
2/3 |
3.4 × 1.6 × 1.5 |
2 |
3 |
1.2 |
1,500 |
2 |
20 |
|
|
|
7 |
4 |
5.4 × 1.8 × 2.0 |
2 |
2 |
1.5 |
1,500 |
2 |
24 |
· Abbreviation: IRE, irreversible electroporation.
· Procedure 4 was performed with 100-μs–long pulses.
Confirmed safety and radiographic determination of lesion response to the initial IRE procedure motivated a series of three additional procedures to treat a total of five lesions over the following 3 months; all of which were performed under general anesthesia with muscle blockade. Figure 1C shows reduced radiodensity surrounding the electrodes corresponding to the region of IRE ablation, including an additional region on the patient's left side from a previous set of IRE pulses. Because of the hepatic capsule puncture–associated pain, all subsequent electrode placements were performed subcostally, which reduced postprocedural pain to a negligible level. Liver function enzymes after the first six IRE procedures showed marked elevation of aminotransferases that resolved in approximately 2 weeks (Fig 2). Conversely, alkaline phosphatase and γ-glutamyltransferase levels remained roughly within normal ranges.
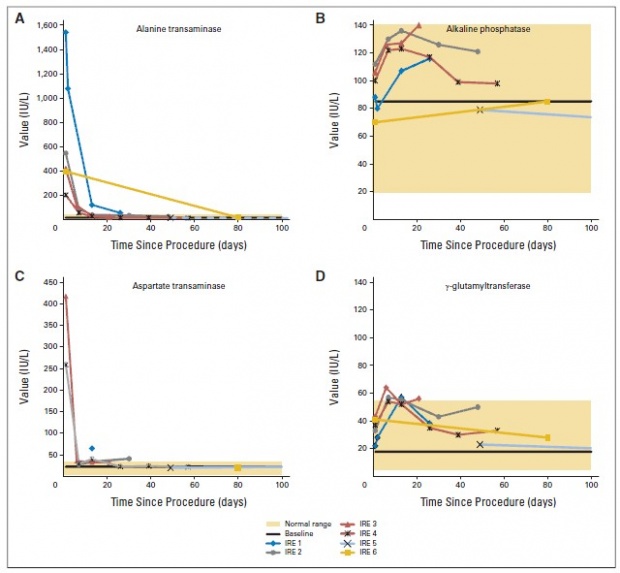
Fig 2.
Serial MR monitoring showed no lesion progression 6 months after IRE, prompting continued follow-up for an additional 6 months of antibiotic therapy.Oncompletion of the second course of antibiotic therapy, the Bartonella infection was not detected in serology or polymerase hain reaction analysis of biopsy samples (in both treated and ntreated lesions). Hematoxylin and eosin staining of core biopsies from the treated lesion (Fig 3D) 2 years after the initial procedure showed normal liver architecture with an increase in chronic inflammation, but no significant interface hepatitis beyond aminor patchy lobular hepatitis.Some fragments presented distorted gland architecture and trabecular thickening with intervening fibrous connective tissue. Hepatocyte nuclei showedminor variation in size, and bile ducts were apparent within the fibrous tracts. Overall, the treated region was consistent with liver with nonspecific inflammation, with no evidence of proliferation of atypical vessels or CD31 immunoreaction. In contrast, an untreated lesion (Fig3A) showed destruction of the normal hepatic architecture and broad bands of fibrous connective tissue that contained proliferating bile ducts and chronic inflammatory cell infiltrate,as well as CD31 immunoreaction(Fig 3B). Scant, short trabeculae of hepatocytes were present within the fibrous connective tissue stroma, and there was a proliferation of CD31 immunoreactive vessels throughout that showed intracytoplasmic vacuolations and tufts. Overall, the features of this untreated lesion were consistent with HEHE.
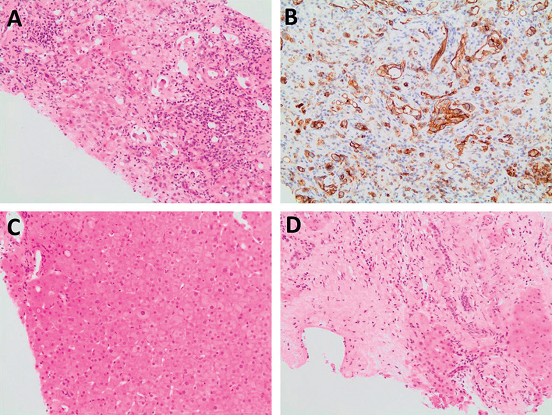
Fig 3
Figure 4 presents CT (A, B), PET (C, D), and composite (E, F) scans of the patient’s liver, showing the first targeted lesion (black arrows) at 12 months before (A, C, and E) and 16 months after IRE ablation (B, D, and F). Although the lesion appears similar in the CT scans (Figs 4A and 4B), a marked decrease in PET metabolic activity is observed (Figs 4C and 4D), which is consistent with the histologic finding of no cancerous cells in the treatment site.
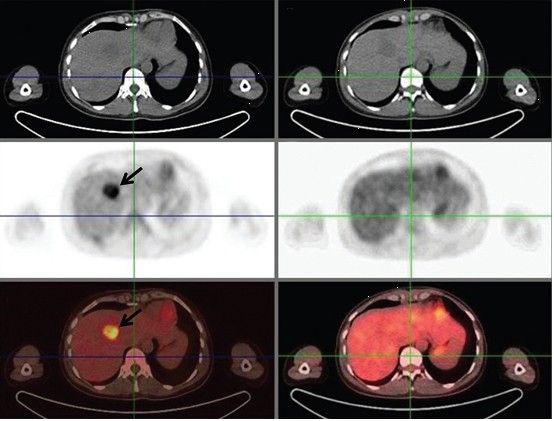
Fig 4
來源:Hepatic Epithelioid Hemangioendothelioma Treated With Irreversible Electroporation and Antibiotics
JCO September 20, 2013 vol. 31 no. 27e422-e426
Prev: 肝門附近的轉移瘤的不可逆電穿孔
Next: 病例報告:肝轉移瘤的不可逆電穿孔
 Follow on Facebook
Follow on Facebook Follow on Twitter
Follow on Twitter Subscribe to RSS
Subscribe to RSS